After Brexit #3
COVID-19 and the Failed Post-Political State
Tara McCormack and Lee Jones
17 April 2020
The British government’s lacklustre response to coronavirus pandemic is not due to “evil Tories” or even austerity. It is a crisis of an entire way of governing society: the post-political, regulatory state.
COVID-19 is supposedly an unprecedented crisis – uncharted territory, akin to the Second World War. The pandemic has hit Britain like a wrecking ball: the economy has been shuttered, Parliament fled for an extended Easter recess, the Queen addressed the nation, and the virus laid low Prime Minister Boris Johnson
Yet, in reality, whatever else this pandemic might be, it is neither unprecedented nor unexpected. It has been part of government security and health planning for over a decade. Why, then, has the state’s response been so chaotic? The truth is that COVID-19 has exposed the frailties of a whole way of governing society: the neoliberal regulatory state, where action plans and reams of “best practice” documentation substitute for the capacity to deliver real public goods.
COVID-19: A Health Crisis Long Foretold
Viral pandemics like COVID-19 are not remotely unprecedented. Pandemic respiratory viruses and even bad flu epidemics kill large numbers with dismal regularity. The 1919-20 Spanish influenza killed 50 million worldwide. The 1957 and 1968-9 flu pandemics killed over 33,000 and 80,000 people in Britain respectively. A particularly bad flu season in 2016-17 caused 28,000 excess deaths.[1] New viral pandemics are different to “regular” flu epidemics as there are no vaccines and no immunity. But clearly it is untrue to say that COVID-19 is something entirely novel.
Indeed, pandemics have been part of government’s security – not merely health – planning since at least the SARS and bird flu pandemics of 2003-4. These outbreaks spurred the World Health Organization to issue revised International Health Regulations in 2005, resulting in widespread global action.[2] The UK’s then Labour government drew up the 2005 UK Influenza Pandemic Contingency Plan, followed by the 2007 National Framework for Responding to an Influenza Pandemic. Under the Conservatives, pandemic disease became part of national security planning. From the first National Security Strategy in 2008 to the 2018 Biological Security Strategy, the government expended unprecedented effort in documenting the likeliness of just such a pandemic and what Britain needed to do.
In 2010, the UK’s second National Security Strategy reiterated that an influenza pandemic was a “tier one” security threat. A National Security Council (NSC), headed by the prime minister, was also established to co-ordinate government efforts and engage in “horizon scanning”, with a sub-committee created to oversee Threats, Hazards, Resilience and Contingencies. The 2011 UK Influenza Pandemic Preparedness Strategy followed, with a “Horizon Scanning Programme” established in 2014. The 2015 National Security Strategy also judged pandemic influenza to be a “tier one” national security risk over the next five-year period, with the risk rising in the medium term. The NHS, which adopted an Emergency Preparedness and Resilience and Response plan, likewise stated that pandemic flu “remains the top risk” for the UK, issuing an Operating Framework for responding to pandemics. In 2018 the Government also published a Biological Security Strategy. Alongside these plans, an alphabet soup of scientific committees were created to advise the government on these matters.
Yet, despite all of these official forecasts and plans, now that this long-anticipated event is upon us we witness general disarray, policy U-turns, rapid improvisation and ad hoc emergency measures. The government appears unable even to ensure that health and social care workers have all the protective gear that they need. How do we explain the mismatch between over ten years of strategic thinking, documents, reports, plans and exercises and the apparent total lack of practical preparation?
We can rule out the possibility that the government’s plans were untested. In 2016 the government “war-gamed” a flu pandemic flu through “Exercise Cygnus”, which revealed a serious lack of preparedness, from lack of personal protective equipment, to ventilators and critical care beds, to oxygen supplies. The government decided not to publicise the results. But Exercise Cygnus was obviously thorough and its findings accurate: we now see the same results playing out in real time.
These findings also refute the claim that governments’ lacklustre response reflects their reliance on a pandemic flu “playbook” which ill-suited the coronavirus. True, COVID-19 is not influenza. But it produces many of the same symptoms, which is why the shortcomings highlighted by Exercise Cygnus are so relevant to the present crisis. The government’s key planning assumptions for pandemic flu are also very similar to the actual conditions experienced with COVID-19.[3]

Austerity seems a more convincing explanation, but even this is not wholly persuasive. To be sure, in 2012, responsibility for public health – non-clinical services concerned with health promotion and protection – was devolved to local governments, which were forced to cut spending by 21 percent from 2009/10 to 2017/18. However, public health is just one part of the multi-agency, “whole-of-government” response envisaged in the endless strategies described above. The NHS, for example, experienced a modest real-terms increase in annual per-person funding of 0.6 percent from 2009/10 to 2016/17.
Moreover, notwithstanding severe data limitations, the available evidence does not suggest a straightforward correlation between healthcare budgets and success in containing COVID-19. Some countries with far lower per capita spending, like South Korea, are more successful than the UK; some with higher spending, like France, are less so.[4] Clearly, as the American case demonstrates most obviously, resources matter – but how they are organised matters, too.

Proper preparation would certainly have required significant additional health spending, though it would have been small beer compared to the costs of the current emergency. Sensible preparations would have included serious stockpiling of personal protective equipment and ventilators (PPE), the creation of reserve testing facilities, and investment in spare industrial capacity to manufacture additional equipment and drugs at short notice. Had these simple preparations been made, the threat of the health service being overwhelmed by treatable cases could have been reduced or eliminated. Closing down most of the economy and imposing an effective state of emergency could have been avoided. A fraction of the resources now being spent propping up the economy could have been concentrated on protecting those at high risk from the disease, while work went into vaccines and treatments.
The state’s failure here is extreme. What caused it?
The Crisis of Regulatory Governance
The real explanation for the yawning gulf between the reams of security planning and actual state performance is the transformation of Western governance over the past four decades. The capacities of the post-war welfare state have been steadily hollowed out, with a shift to neoliberal, regulatory and networked governance. This system is better at creating the illusion of activity than actually delivering concrete public goods and services. This has left political elites scrambling for an emergency response, in which controlling the population substitutes for providing for them. In this sense, COVID-19 is the epitaph of a whole way of organising our collective political life.
The post-war welfare state, whatever its manifold flaws, had the merit of a very clear “command-and-control” system, which grew out of the massive mobilisation of people and resources required in World War 2. The state engaged in detailed social and economic planning, nationalising resources and establishing national and local bureaucracies as required to deliver goods and services directly to the public.
During the crisis of the early 1970s the capitalists realised that they could no longer tolerate the post-war order because it undermined their control of the economy. Under Margaret Thatcher, their power was restored, and the state retooled accordingly. Planning was abolished, bureaucracies disestablished, state-owned enterprises privatised, and provision of goods and services increasingly outsourced to the market.
Authority was also radically dispersed in what academics often call the shift from government to governance. Policymaking was increasingly outsourced to tens of thousands of public and private regulators, from quasi-autonomous non-governmental organisations (quangos) to independent central banks. Responsibility for providing public goods – though less so the resources needed to provide them – was decentralised to devolved administrations and local governments. “Partnership working” drew businesses, charities and others into an increasingly complex “governance” network. The role of central state apparatuses shifted from providing authoritative decisions to merely issuing regulations designed to steer this complex array of agencies towards broadly desirable ends.
As well as fragmenting internally, the regulatory state’s power and responsibilities were also diffused upwards and outwards, through hundreds of international agencies. The European Union was the sine qua non, with decision making across vast swathes of public life shifting away from national governments and parliaments to transnational politico-bureaucratic networks. But this was increasingly mirrored worldwide, as national regulators networked across state borders to develop “best practice” codes, then cascade them downwards into their national contexts.
This transformation in the nature of state power is experienced by ordinary citizens as a dramatic weakening of their control over their social, economic and political lives. When authority is so dispersed, vertically and horizontally, it dissipates. It becomes hard to pin down exactly who is responsible for what, and much easier for authorities to shift blame around and avoid accountability. The main mechanism through which citizens influenced the post-war state – voting – becomes decreasingly meaningful as policy decisions are no longer made publicly, in national parliaments, but are outsourced to unelected technocrats or are determined behind closed doors in mysterious “stakeholder partnerships”, sometimes spanning several continents. Policy options offered at elections contract markedly as public life is managed according to a new technocratic consensus, and politicians spend more time explaining why things simply cannot be changed than articulating alternative visions of the future. The transformation of nation-states to member-states in Europe is merely the most obvious manifestation of this uneven global trend, against which populations are now beginning to revolt.
The Regulatory Governance of Global Health and Security
British health and security policy, which now intersect, reflect these transformations in the nature of state power.
After WW2, British security policy was narrowly contained within Cold War parameters, implemented by a tiny handful of agencies (notably the Foreign Office and Ministry of Defence), and enjoyed cross-party consensus. It was, in effect, de-politicised, reflecting the existential stakes of mutually-assured destruction. Since the Cold War, however, security has become subject to much greater political and bureaucratic contestation, much like any other policy domain. Elites’ ability to clearly specify Britain’s “national interest” and, by extension, prioritise its security agenda, has withered. Britain became mired in fruitless overseas interventions, while security policy bloated to incorporate “non-traditional” threats and risks, from disease to terrorism to environmental degradation, drawing in a host of other bureaucratic agencies and interests.
The creation of the National Security Strategy (NSS, 2008) and National Security Council (NSC, 2010) represented efforts to cohere this increasingly aimless and messy policy space. After initially providing little more than a laundry list of challenges, subsequent iterations of the NSS moved towards clearer priorities. The NSC, meanwhile, seeks to coordinate the many different agencies now involved in security, spurring them to develop relevant action plans and guidelines, which are then supposed to be implemented across relevant departments and agencies.
Ironically, however, the NSC’s own structure reflects the fragmentary and diffuse nature of regulatory statehood. Ostensibly chaired by the prime minister, the NSC has four sub-committees: Threats, Hazards and Resilience, which deals with health security (supported by several scientific advisory committees); Nuclear Deterrence and Security; a sub-committee to implement the Security and Defence Review; and the Cross-Government Funds Committee. The National Security Advisor is simultaneously the Cabinet Secretary (currently Sir Mark Sedwill), who has to manage the entire Home Civil Service. The National Security Secretariat is supposed to coordinate security and intelligence matters across government, but so is the Joint Intelligence Committee. The evident difficulty of coordinating this “whole-of-government” approach to security was expressed in Sedwill’s “fusion doctrine” in the 2018 National Security Capability review. This promoted a “whole-of everything” approach, aspiring to “fuse capabilities across ‘economic, security, social and the rest’, to deliver strategy-led design of policy and planning”.
Authority and policymaking has also diffused upwards to global bodies – like the World Health Organisation (WHO) in the realm of global health security. However, Contrary to right-wing claims of an emerging “world government”, the World Health Organisation (WHO) has no direct, sovereign power to manage global health. In fact, the WHO’s capacities have themselves been steadily hollowed out by the neoliberal revolution and it, too, relies on regulatory modes of governance.
The WHO used to focus on building up post-colonial countries’ public health systems and eradicating preventable diseases. But since the 1980s, powerful donor states have stripped the WHO of much of its core budget, constraining it to work in project-based, “siloed” manner, mostly targeting communicable diseases of concern to wealthy, Northern states. Alongside the World Bank and others, the WHO also shifted towards promoting private-sector healthcare in developing countries. These changes have weakened the WHO’s autonomy from wealthy states, making it highly unreliable in times of crisis, lurching between alarmism in a desperate attempt to mobilise resources, while also seeking to avoid alienating powerful member-states, like China. Meanwhile, much of its remit has been usurped by unaccountable private and philanthropic bodies like the Bill and Melinda Gates Foundation.
Now, rather than directly helping to build healthcare capacity in member-states, the WHO mostly tries to regulate health security by specifying how domestic laws, institutions and processes should operate. The WHO’s 2005 International Health Regulations (IHRs) exemplify this approach. Developed by a committee of unelected technocrats, the IHRs closely specify what countries should do in order to contain pandemic diseases. Member-states are then tasked with implementing the IHRs domestically, by transforming domestic governance accordingly. The endless documents generated by the British government since 2005 on pandemic preparedness are the paper trail of the UK’s compliance.
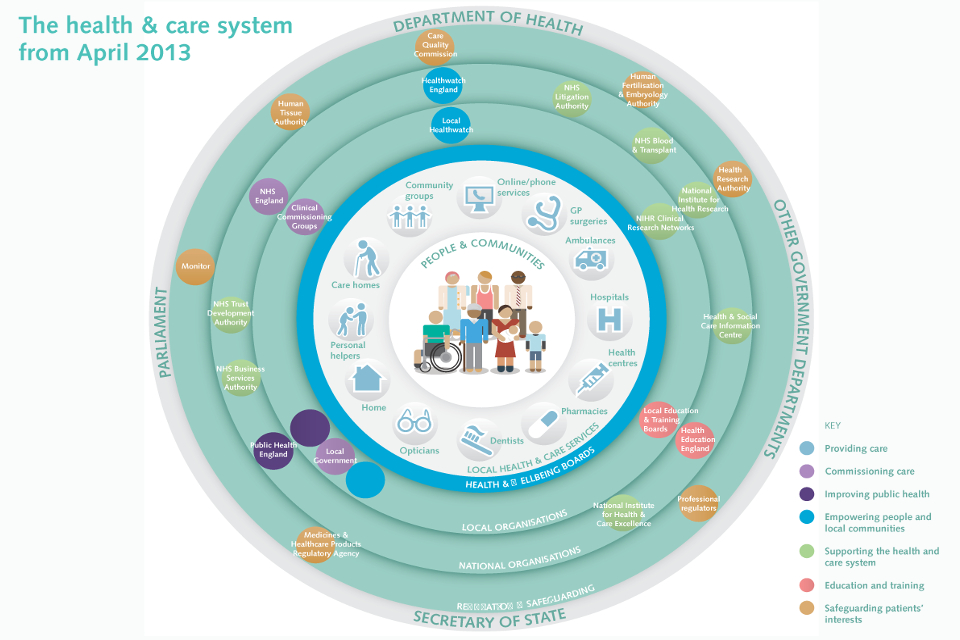
However, these global regulations are being cascaded through institutions which themselves have been transformed by the shift to regulatory statehood. This is true not merely of the UK’s NSC, but other state apparatuses too – including, most pertinently, the NHS. Understandably, the average citizen still believes that “the government” is “in charge” of healthcare; the Department of Health and Social Care “runs” the NHS and, if things go wrong, the Secretary of State is accountable. In reality, this traditional command-and-control system was long ago replaced by an incredibly complex array of public and private actors without clear lines of authority and accountability (see diagram below). The Department of Health is no longer “directly involved in operational matters and relies on Arms-Length Bodies who commission and regulate care”.[5]

Look inside any of the agencies listed in this diagram and you will discover a similarly Byzantine internal governance structure, with devolution adding additional complexity. This, for example, is the Welsh system.

The traditional hierarchy represented in these organograms, with parliaments notionally at the “top” is positively misleading. In the English NHS, decisions about what healthcare to actually provide, and how, are actually made by the lowest “rung” on the ladder, “clinical commissioning groups” (CCGs). These CCGs, which took over from Primary Care Trusts in 2012, have a similarly confusing network structure, as this example from Northamptonshire shows.

Indeed, instead of hierarchical organograms, a relic of the “command and control” welfare state, in the regulatory state it’s more common to see governance arrangements described as flows or circles, where no one is really in charge and accountability is so dispersed as to be effectively meaningless.
As global and national regulations on health security are cascaded downwards into this “system”, each agency may generate its own bureaucratic action plan, but responsibility becomes remarkably diffused. Bureaucracy proliferates, with regulators always seeking to regulate someone else, who is actually responsible for undertaking concrete, practical activity. It becomes increasingly difficult to know who is responsible for what, to check that key actions have actually been undertaken, and to assure that fragmented activity actually adds up into a coherent whole.
COVID-19: The Chickens Come Home to Roost
As COVID-19 demonstrates, this governance system is far better at producing reams of well-meaning documentation, regulations and best-practice guidelines, spanning a whole range of “stakeholders”, than actually making the concrete preparation required to withstand a pandemic. The crisis clearly calls for hierarchical, “command-and-control” systems, which now have to be improvised out of thin air.
From the outset, the government’s haphazard response to COVID-19 has reflected the outsourcing of decision-making to technocrats in a fragmented governance regime. Despite media attacks to the contrary, the UK government really does seem to have been “guided by The Science” (sic) from the very beginning, with the alphabet soup of advisory committees activated and the chief medical and scientific officers rising from obscurity to become household names.
Yet it transpires that The Science is not actually a viable substitute for political authority, for two reasons. First, particularly when confronted with a novel phenomenon like a new virus strain, science is not a single, coherent body of knowledge but rather an evolving practice of hypothesis-testing in a context of very uncertain data. Scientists have produced wildly varying estimates of the spread and lethality of the virus. The WHO announced a death rate of 3.4 percent in early March; recent papers from Germany and US suggest rates of 0.4 and 0.66 percent respectively. Certainly, early suggestions that the COVID-19 was serious in a fifth of cases and critical in five percent of them do not seem borne out by the European experience. Similarly, an Oxford University team suggested that perhaps half the population could already be infected, which was vigorously disputed by a UCL team. Having outsourced its authority to scientists, the UK government’s response to COVID-19 has thereby been buffeted around by the latest scientific modelling. The current lockdown stemmed from a panicked reaction to an Imperial College study warning of 510,000 deaths without stricter containment measures.
The second reason why outsourcing authority to “the experts” is problematic is that the experts themselves actually continue to defer to the traditional wielders of authority. The government’s scientific advisers do not simply present the untrammelled “truth” of the situation and instruct ministers on what to do. Rather, they factor what they take to be political realities into their advice, warping it from the outset. As a detailed Reuters investigation found, scientists were slow to recommend stricter containment because they did not believe a lockdown would be politically acceptable. “We didn’t model it because it didn’t seem to be on the agenda”, one said. That only changed when the lockdown in Italy “opened up the policy space”.
It also seems clear that the government’s “science-led” policy was always warped around the state’s utterly inadequate material preparations. The UK could never have pursued a Korean-style track-and-trace approach – so far the world’s most successful response to COVID-19 – because it lacked (and still lacks) the required capacity for mass testing, let alone the digital tracking systems required for contact tracing and targeted quarantine enforcement. The government’s so-called “delay” phase, which relied on testing and contact tracing, was mostly for show, with testing rationed to high-risk cases, allowing the disease to spread unmonitored among mildly affected or asymptomatic individuals.
The lack of basic stockpiling also denotes a state more comfortable with bureaucratic coordination and stakeholder partnerships than actually taking concrete measures to protect the public. Consider the issue of personal protective equipment (PPE). On paper it looks as though the state has responded impressively, delivering 158 million masks, a million gowns, 135 million aprons, and 360 million pairs of gloves since the end of February. However, this has exhausted its stockpiles. Even before the peak of the pandemic, intensive care unit staff are reporting shortages, NHS staff on wards are having to make aprons out of bin bags, and social care workers are hardly protected at all, despite care homes reporting cases in a third of their institutions. The government is already rationing scarce PPE while implying that healthcare workers are to blame for using it inappropriately.
This state failure is also symptomatic of the material shifts underpinning the transformation in state power, notably the globalisation of capitalist production. The shift to regulatory statehood was primarily about facilitating this development, promoting global competitiveness over national development. Having accepted Britain’s transition into a post-industrial economy, the political elite suddenly find themselves competing on global markets for PPE and other vital equipment like testing kits and ventilators. Conversely, states that have resisted de-industrialisation, like South Korea and Germany, have greater domestic supplies and industrial capacities that could quickly be repurposed to produce key equipment.
Importantly, this state failure goes right down to the local level, where the hollowing out of state capacity, and the replacement of public services with a patchwork of voluntary and private services, has left millions of people highly vulnerable to the virus. Reflecting regulatory state practices, local officials have hurriedly improvised familiar networked arrangements between these different entities (see diagram below for an example in London). But, as usual, these are more impressive on paper than in practice.

Councils, overwhelmed by demands on their services, have tried to outsource responsibility to local “charitable and voluntary sector” (CVS) hubs, which will supposedly fill the vast holes in Britain’s threadbare social safety net by deploying volunteers and charities. Yet these CVS hubs are often threadbare themselves – perhaps just five full-time staff trying to improvise a pandemic response across boroughs of 400,000 people. They are desperately short of people to actually undertake practical activity – to deliver concrete goods and services. Crates of food are being dumped at CVS hubs without any clear sense of who should get them or how, and without the necessary personnel to even deliver them. CVS officials complain that council bureaucrats are generating reams of “best practice” guidelines, but few are providing the actual “stuff” that people need. In the regulatory state, it is regulators all the way down.
This has shunted a frightening amount of the practical burden of caring for people through the pandemic onto a motley army of volunteers. At a local level, mutual aid networks have been hastily improvised to plug the gaps in the system – some gaining grateful support from visibly relieved officials, others facing active sabotage by local councillors. Nationally, some 750,000 people volunteered to help the NHS get supplies to the most vulnerable individuals, then languished for weeks while national bureaucrats scrambled to assemble lists of these individuals from scratch and find ways to deploy the volunteer army. Still, there is immense confusion between national and local state and voluntary organisations about who is covered by what arrangement, with many impoverished people continuing to slip through the net.
The COVID-19 crisis clearly demands a return to a more interventionist, command-and-control system, but the British government’s cack-handed approach demonstrates the difficulty of reinventing this on the hoof. In response to a woeful lack of ventilators, the government demanded that manufacturers build 20,000 units using novel designs relying exclusively on UK supply chains. In a sign that the attitudes around the regulatory state are slow to change, many manufacturers reacted sniffily, insisting that it simply couldn’t be done. Ultimately, however, with much fanfare the government selected Dyson – which had never previously manufactured ventilators – to “get it done”.
Ostensibly impressive – until one notes that existing British ventilator manufacturers, with whom foreign governments were already in touch, had not even been approached by the government. A month later, the government has still only been able to procure 13 percent of its target. UK testing kit manufacturers were similarly neglected, with the government instead ordering 17.5m kits from overseas that quickly turned out to be useless. Laboratory operators have expressed similar bemusement that their offers to help conduct testing have been ignored, with Public Health England ploddingly insisting on centralised testing in Milton Keynes, resulting in one of the worst regimes in the developed world.
Conclusion: Can Britain Re-Learn the Art of Government?
The COVID-19 pandemic is not simply a public health crisis. Perhaps more importantly, it is a crisis of a whole way of governing society. The shift to regulatory statehood and transnational governance has hollowed out the practical capacities needed to respond meaningfully to genuine threats to public welfare. From being a Hobbesian Leviathan to whom citizens defer in exchange for protection, the state has become an enfeebled coordinator of multi-sectoral partnerships, desperately trying to protect itself from the public: “stay home – protect the NHS – save lives”.
Western governments’ faltering responses to the pandemic re-poses a question already raised by Brexit: can we re-learn the art of government, as opposed to governance? For those still mired in the regulatory regionalism of the European Union, the outlook seems dismal. After weeks of wrangling, ministers failed to agree meaningful burden-sharing, clinging fiercely to neoliberal dictums. Italy can borrow more, but beyond two percent of GDP any use of this additional credit for healthcare will trigger neoliberal conditionalities. Meaningful action has been left to individual European states, mostly as ill-suited to improvising command-and-control systems as Britain – and locked into Euro-austerity to boot. Little wonder that Euroscepticism is increasingly sharply in the ravaged countries of southern Europe.
What of Britain? Johnson’s populist slogans “take back control” and “get Brexit done” resonated precisely because they spoke to the frustration ordinary citizens felt when confronted by opaque and unresponsive regulatory governance. They promised to just cut through all the bureaucratic blather to deliver outcomes demanded by the public. That determination was also reflected in the Tory manifesto, which promised a far more interventionist state.
Yet, as previously argued on The Full Brexit, this requires a political will and institutional innovations long abandoned by our politicians and civil servants (see Analysis #48 - How Will the Tories Rule? Understanding Boris Johnson's Political Project). The COVID-19 pandemic illustrates starkly the difficulty of unpicking decades of state transformation.
To be sure, there are some hopeful signs. For instance, the Bank of England’s initial resistance to directly financing the government’s COVID-19 spending – a hangover of the neoliberal order – was swiftly overcome. Having effectively converted to Modern Monetary Theory, the Bank is now effectively printing money to finance the crisis, and thus behaving more radically than the “Marxist” former shadow chancellor John McDonnell, who instead called for higher taxes on the wealthy.
Similarly, the volunteer army’s emergence shows a reluctance among millions of citizens to simply “stay at home”. This is an important and moving break from neoliberal norms, which actively encouraged a demoralised citizenry to retreat into private life and consumption. It is all the more impressive in the context of a pandemic in which a neighbour one wants to help could be carrying a deadly disease.
The volunteers put to shame our political representatives at Westminster who, by contrast, could barely wait to retreat from public life. The sustained leeching of power away from parliament in the regulatory state has led our legislators to forget their vital role in representing the people and holding the executive to account. By rising early for an extended Easter recess, having just waved through sweeping authoritarian powers without a vote, speaks to a profound lack of responsibility, an unwillingness to take back control (see After Brexit #1 - COVID-19: We’re Not In Control).
The idea that the COVID-19 response is not a political matter and “now is not the time” for politics is completely mistaken. Decisions about how we allocate resources and respond to significant problems are always fundamentally political. It is at exactly at times of crisis, and especially when granted unprecedented peacetime powers, that government needs to be held to account. Above all, the post-political state as such has failed. It is exactly at this time that we need to be thinking urgently about how to replace it.
References
[1] Figures from the UK government’s coronavirus action plan.
[2] See Shahar Hameiri and Lee Jones, Governing Borderless Threats: Non-Traditional Security and the Politics of State Transformation (Cambridge: Cambridge University Press, 2015), ch.4. Parts of this article draw heavily on this book.
[3] Cabinet Office, Preparing for Pandemic Influenza: Guidance for Local Planners (London: HMSO, 2013), p. 16.
[4] Healthcare spending is for 2017, from the WHO’s Global Health Expenditure Database, denominated in US dollars adjusted using 2011 purchasing power parity rates. Coronavirus data as reported on 14 April 2020 by Worldometers.com.
[5] National Assembly for Wales, The organisation of the NHS in the UK: comparing structures in the four countries (Cardiff: National Assembly for Wales), p.10.
About the Authors
Dr Tara McCormack is Lecturer in Politics and International Relations at the University of Leicester and author of Britain’s War Powers: The Fall and Rise of Executive Authority? (London: Palgrave 2019). Dr Lee Jones is Reader in International Politics at Queen Mary University of London and co-author of Governing Borderless Threats: Security Governance and the Politics of Non-Traditional Security (Cambridge: Cambridge University Press, 2015). They are both co-founders of The Full Brexit.
This work represents the views of the author only. It is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.